Internal impingement
Posterior impingement
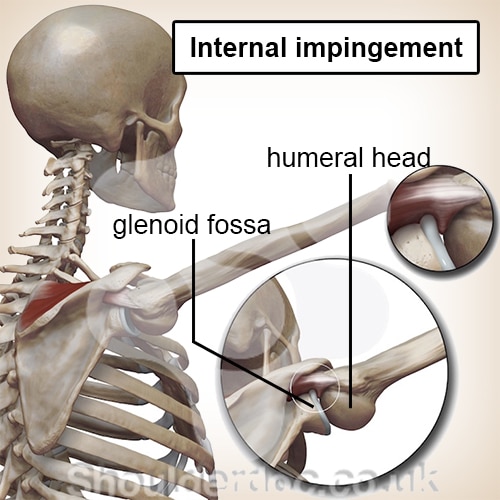
An internal impingement is an entrapment of tissue between the humeral head and glenoid fossa. The symptoms are mainly felt during overhead sports activities, such as overhead throwing. It is therefore one of the most common shoulder complaints in overhead sports.
This disorder is also referred to as internal impingement and posterior impingement.
Description of the condition
The shoulder joint consists of a humeral head and glenoid fossa. The humeral head is the end of the upper arm, the glenoid fossa is a concave recess of the shoulder blade. The (acromion) sits above this recess. The shoulder muscles (rotator cuff muscles) ensure that the humeral head can move in the glenoid fossa. These muscles also ensure that the humeral head stays in the cavity.
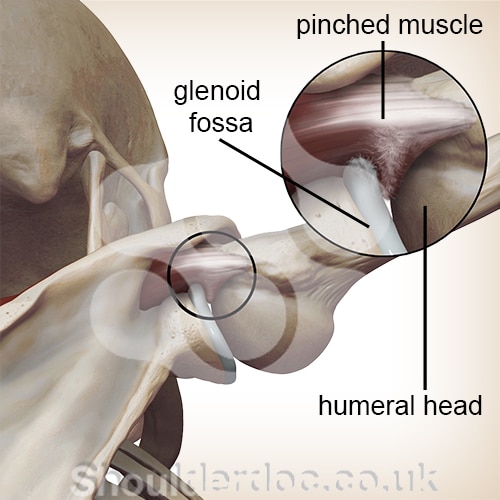
In case of an internal impingement, the shoulder muscles at the rear of the shoulder are wedged between the humeral head and glenoid fossa. Especially in the position in which a ball is thrown overhead. In this position, the tendon of the infraspinatus and/or supraspinatus muscles get wedged.
Cause and origin
Internal impingement occurs mainly in overhead sportsmen. The throwing movement plays an important role in this. During throwing - or other overhead sports activities - enormous mobility and stability is required from the shoulder joint. As a result of the frequent throwing, the mobility of the shoulder used for throwing is often slightly greater than the shoulder of the non-throwing arm.
The cause of internal impingement is multifactorial, which means that several factors play a role in its occurrence. These factors can be:
- Anterior instability of the shoulder.
- Increased tension in the back of the shoulder.
- Reduced control of the shoulder blade.
- Incorrect technique.
- Excessive strain.
- Influence on the entire body (kinematic chain).
Due to anterior instability, more space gets created at the front of the shoulder capsule. During the act of throwing, the humeral head rolls and slides toward in the cavity. In case of instability, the humeral head can slide too far forward. When the humeral head moves too far forward, extra space gets created in the back. The muscles can get impinged in this space.
In addition, the rear of the shoulder capsule is often taut. As a result of this tension, the humeral head is pushed forward. This shift can again cause instability in the front.
It is remarkable that both instability in the front and tension in the back of the shoulder develops in every overhead athlete. In other words, this happens in both those with shoulder complaints and those without. That is why it’s the other factors that cause these characteristics to give complaints.
Signs & symptoms
The most frequently mentioned complaints are stiffness when throwing and pain at the back of the shoulder. It is also often noted that there is a loss of performance. This loss can be experienced in terms of speed, strength or coordination. The complaints are triggered by the sporting activity. Usually, the complaints are not present in daily life.
Internal impingement can be divided into three stages:
Stage 1
A feeling of stiffness in the shoulder and a longer warm-up period is needed to get warm. There is no pain present.
Stage 2
Complaints as in stage 1, with pain now being present during overhead sporting activities. There is no pain in day-to-day activities.
Stage 3
Complaints of pain and stiffness are present during sporting and daily activities, even after a period of rest.
At the time of the physical examination, an increase in mobility is observed when rotating the arm outward (exorotation) and reduced mobility when rotating the arm inward (endorotation).
Diagnosis
The diagnosis is made on the basis of an interview and physical examination. Additional testing is not necessary to diagnose internal impingement.
If there is any suspicion of injury to the labrum, additional testing is recommended. The labrum is a ring of connective tissue that lies on top of the glenoid fossa. A labrum injury in combination with internal impingement occurs regularly. If the labrum is damaged, it can become wedged (SLAP lesion). To rule this out, an MRI is performed.
Treatment
The treatment of internal impingement is in most cases non-surgical (conservative). The stage of internal impingement is important to get the right treatment. In addition, the cause will have to be examined.
The treatment in stage 1 is usually sufficient with rest and possibly anti-inflammatories. In stage 2, the patient will have to maintain (relative) rest for at least six weeks and physiotherapy will play an important role in the treatment. The treatment in stage 3 is the same as in stage 2, but with a longer period of (relative) rest.
The physiotherapeutic treatment focuses on correcting the mobility and stability of the entire shoulder complex. The shoulder complex includes: the shoulder joint, the shoulder blade and the top part of the spine.
In addition, the focus will be on the entire kinematic chain and the technique will be reviewed, possibly in collaboration with the trainer/coach.
Injections in the shoulder joint do not provide any added value in the treatment of internal impingement. Surgical treatment of internal impingement is only necessary when this is caused by another shoulder disorder. For example, a SLAP lesion.
Exercises
Follow the exercise programme with exercises for the internal impingement of the shoulder here.
You can check your symptoms using the online physiotherapy check or make an appointment with a physiotherapy practice in your area.

References
Corpus, K.T., Camp, C.L. Dines, D.M., Altchek, D.W. & Dines, J.S. (2016). Evaluation and treatment of internal impingement of the shoulder in overhead athletes. World J Orthop 2016 dec:18; 7(12): 776-784.
Jansen, M.J., Brooijmans, F., Geraets, J.J.X.R., Lenssen, A.F., Ottenheijm, R.P.G., Penning, L.I.F. & Bie, R.A. de (2011). KNGF Evidence Statement. Subacromiale klachten. Jaargang 121. Nummer 1. 2011.
Manske, R. & Ellenbecker, T. (2013). Current concepts in shoulder examination of the overhead athlete. Int J Sports Phys Ther. 2013 Oct;8(5):554-78.
Nugteren, K. van & Winkel, D. (2007). Onderzoek en behandeling van de schouder. Houten: Bohn Stafleu van Loghum.
Wilk, K.E., Reinold, M.M. & Andrews, J.R. (2009). The atlete's shoulder. Philadelphia: Churchill livingstone. Elsevier.